A Patient Story: Treating Dupuytren’s Contracture with Low-Dose Radiation Therapy
By: Adrian Treverton, Xstrahl CEO, written during and after his own course of treatment

I walked into my first consultation knowing exactly what was going to happen. After more than twenty years in radiation therapy, building a company around these systems, standing in treatment rooms, and talking to physicians about beam quality and workflow, there were not supposed to be many surprises left for me. This time, though, I was the patient, and that changed everything.
Perspective Changes Everything
Even with all that experience, I felt nervous sitting in the waiting room on Day 1. Not because I did not understand the process; I understood it too well. I found myself asking the same questions every patient asks: what if the diagnosis is something worse, how will this affect my schedule, will I need to change how I train or work or live? The waiting room itself was the biggest shift. You stop seeing patients and start seeing people. Conversations about treatment, side effects, children, and holidays; real lives being lived around a diagnosis.
Most of the people around me were facing something far more serious than I was. I was there for a benign condition, Dupuytren’s contracture, the progressive thickening of tissue in the palm that can pull fingers into a permanently bent position. They were fighting cancer. My sister once told me that as a nurse you just see patients, but as a patient you see other people. Sitting in that corner, grateful and a little guilty, not fighting for my life or wondering how much time I had left, that observation had never felt more true.
“My sister told me that as a nurse, you just see patients. But as a patient, you see other people.”
The Diagnosis and the Decision
Dupuytren’s contracture is not rare, but it is underappreciated. The nodules and cords that form beneath the skin can progress slowly over years, and by the time the condition becomes noticeably limiting, many patients are already being referred straight to surgical intervention, typically a fasciectomy to remove the thickened tissue. I had known about my own condition for a couple of years before deciding to act. After consulting with a specialist in Germany, the recommendation was clear: radiation therapy first, and for one larger nodule, possible surgery followed by post-operative RT. The goal was to slow or halt the progression and, ideally, avoid surgery altogether.
Being self-referred brought its own complications. At fifty, I was not covered the same way many older patients are under Medicare, and navigating the insurance landscape made me realize just how much the system can work against patients, even those who understand it from the inside. It gave me a fresh perspective on the reimbursement conversations we have internally. We often think about reimbursement in terms of justifying equipment investment, but sitting on the other side of that equation, it became very clear how directly those decisions affect the people we are actually here to help.
The Reality of Treatment
The treatment itself was straightforward: low dose, quick, and efficient. Twenty-six seconds on beam per session, with both hands treated in a single visit. There was no drama, no pain, and no immediate side effects beyond a little warmth in my hands that I was fairly sure was psychological. If anything, the simplicity almost works against it, because you stand there with your palm facing upward and think, is it even doing anything? That simplicity is exactly the point. Radiation therapy for benign musculoskeletal conditions like Dupuytren’s is one of the more elegant interventions in medicine: non-invasive, targeted, and low-burden on the patient. My hands were a little dry over the weeks of treatment, a side effect I was more inclined to attribute to cold weather than to radiation, though I know the effects operate on a delayed timeline through DNA damage and repair pathways.
What stood out to me more than the technology was everything around it. The early mornings, the thirty-minute drive, the rearranging of a schedule to make each fraction on time. Over ten sessions across two rounds, the logistical commitment accumulates, and it made one thing very clear: access matters just as much as efficacy. When I was tired and rushed on a Friday morning for my last fraction, thinking about whether the treatment would even work, I was not thinking about beam quality. I was thinking about getting through the day.
“The treatment doesn’t hurt. People in the waiting room probably wonder if the machine is even on, though the alarm going off tells you it is.”
What Patients Actually Experience
In our industry, we talk about dose, fractionation, beam quality, shielding, and workflow. These are important things. But patients do not experience any of them the way we do. They experience the inconvenience of getting there, the uncertainty of whether it will work, the financial impact of how it is reimbursed, the relief when the machine is running and the frustration when it is not, and above all the quality of the human interactions along the way. One moment stuck with me particularly: on treatment day five, I realized that if I had arrived and been told the machine was down, I would have been genuinely frustrated, not as an industry professional, but as a patient who had rearranged their morning to be there. That is the point at which uptime stops being an operational metric and becomes part of patient care.
I also noticed the small things that quietly shape a patient’s experience. The nurse who explained that the effects linger in the body was not being technically precise, but it was a kind way of conveying that recovery takes time. The waiting room becomes a small community, where strangers compare notes on metallic tastes during chemotherapy and share stories about their families. And then there is the uncertainty that sits with you between fractions, quietly asking what happens if it does not work. These are the things patients are actually navigating, and they are worth understanding if we want to build systems and services that genuinely serve them.
A Better Path Forward for MSK Patients
This experience reinforced something we have believed for a long time: MSK radiation therapy is underutilized, and the barrier is access rather than efficacy. The treatment works. Compared to surgery, the case is compelling: no incision, no meaningful recovery time, minimal side effects, and a lower overall cost burden on the system. And yet patients frequently end up on the surgical path because that is what is available, what is reimbursed, or what their referring clinician knows to offer. Even as someone inside the industry, with the knowledge and connections to navigate the system, I encountered real insurance challenges, referral complexity, and logistical friction. If it is that difficult for me, it is worth asking what that experience looks like for patients who do not have that background.
Reading surgical horror stories on patient forums while waiting for my second round of treatment, I felt the weight of that access gap more acutely. Many of those patients had no idea that a non-surgical option existed. I found myself regretting not starting treatment two years earlier, though at least I had found my way there. Not everyone does.
“I found myself regretting not starting treatment two years earlier, though at least I had found my way there. Not everyone does.”
A Final Thought
Walking out after my final fraction, I felt genuinely elated. The treatment was over, yes, but more than that, the whole experience had given me a completely different lens on the work we do. I had read the horror stories about surgery. I had sat in waiting rooms full of people dealing with things far harder than mine. And I had experienced firsthand, without any professional distance to hide behind, what it actually feels like to be on the receiving end of the care we help make possible. That matters. The goal of this work, properly understood, is to make treatment simpler, more accessible, and more human. If we get MSK right, we have the opportunity to change how an entire category of patients is treated and to spare many of them from the surgical path they are currently told is their only option. That is worth building for.
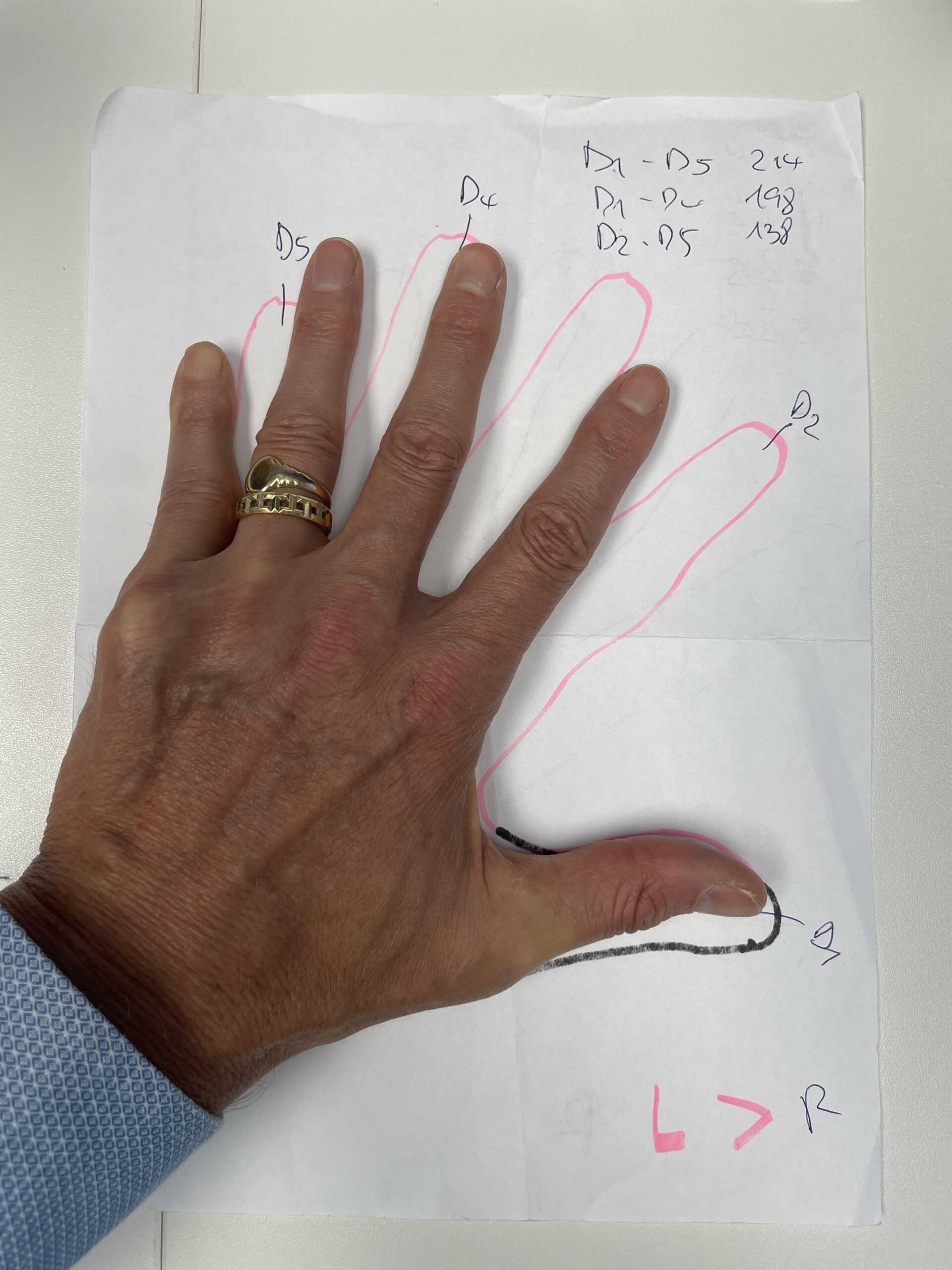
Pictured: Before and 6 Months After Treatment
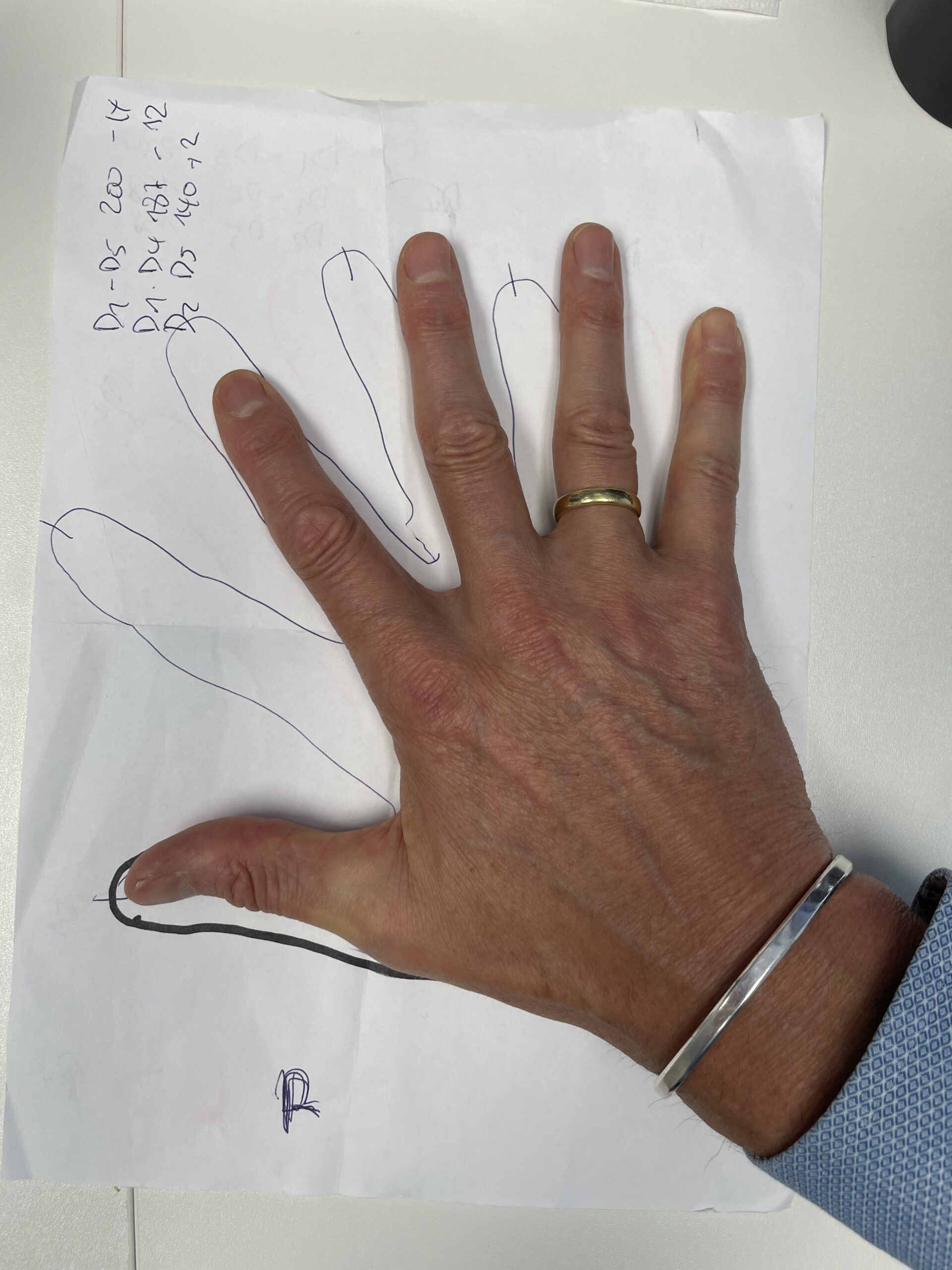
About Dupuytren’s Contracture
Dupuytren’s contracture is a progressive fibrotic condition affecting the connective tissue of the palm. Nodules and cords form beneath the skin and can gradually pull one or more fingers into a permanently flexed position. It is more common in men over 40, those of Northern European descent, and individuals with a family history of the condition. Low-dose radiation therapy has been shown to slow or halt disease progression, particularly in the early stages, and is a well-established non-surgical treatment option in Europe.
If you’re considering adding LDRT to your clinic, we’d welcome the conversation. Whether you’re at the early research stage or ready to look at what implementation actually involves, Xstrahl’s team has the clinical and practical experience to walk you through it, from patient selection and fractionation protocols to equipment, reimbursement, and workflow integration.
Request more information here.